Live today — built & usable now
Live, enhancement on deck — core works; we extend the gap
On the build plan — scoped with a timeline
~1 wk 2–4 wks 1–2 mo build effort
Recently completed
Even more of your list is now live.
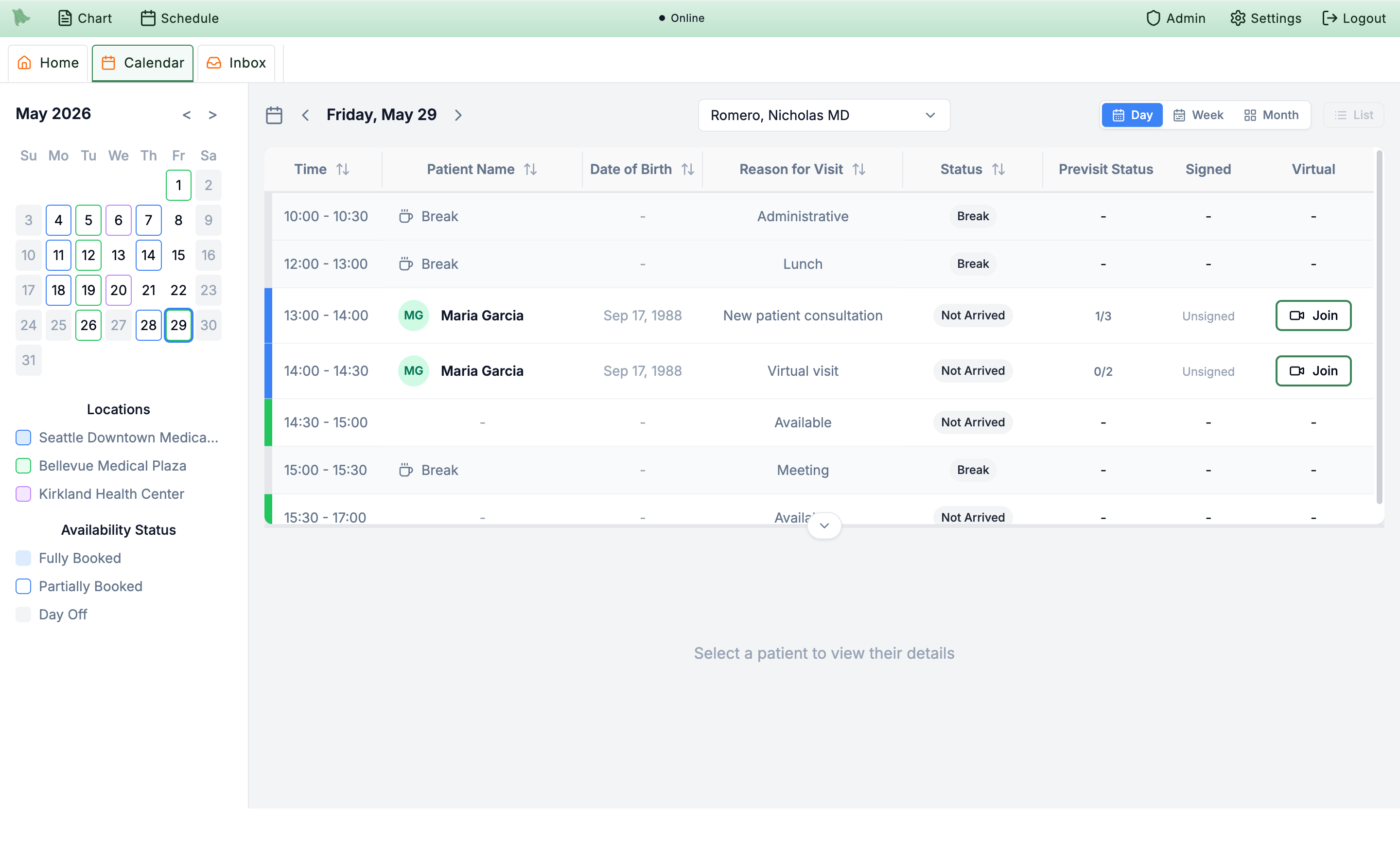
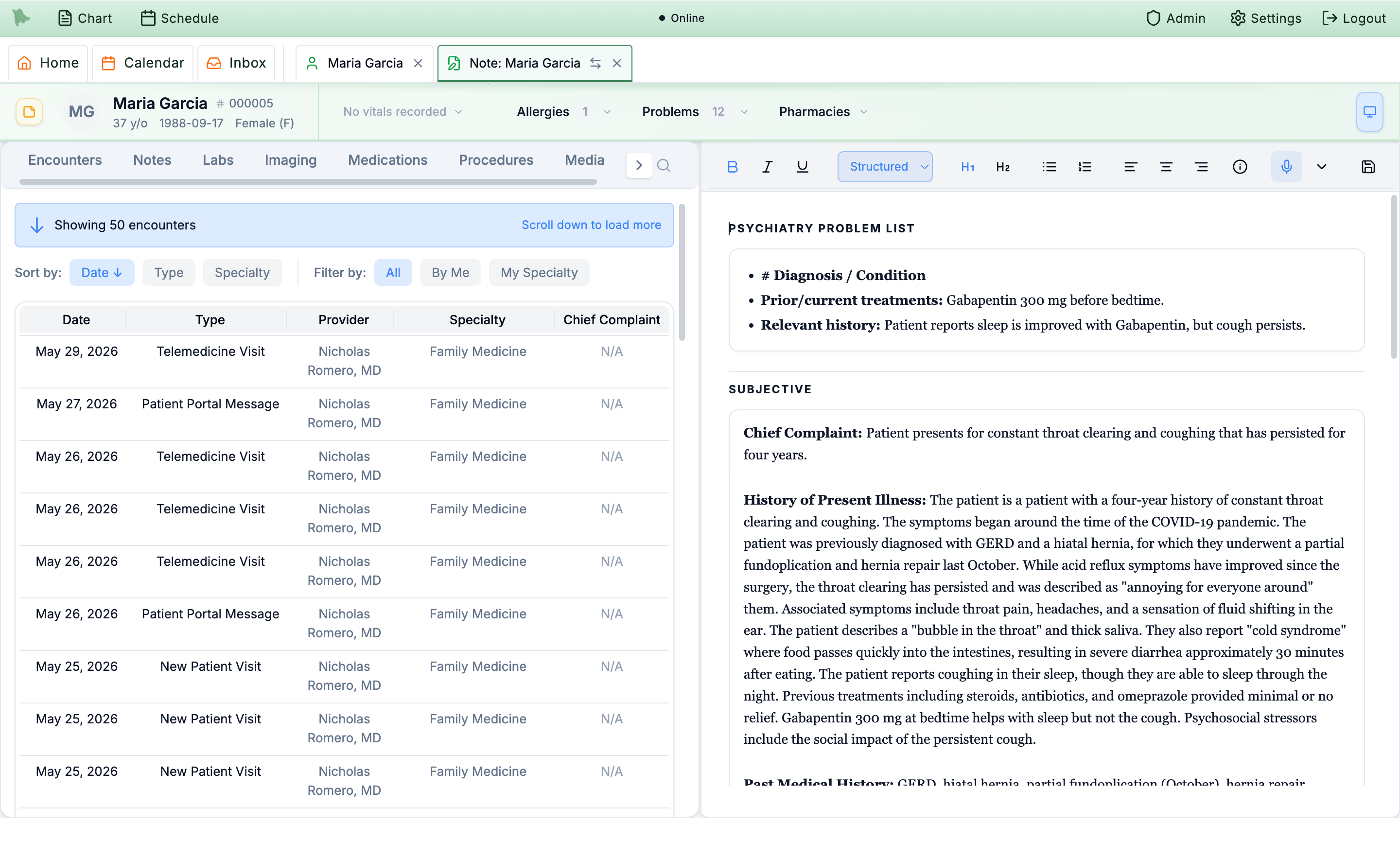
Clean exportable scheduleCalendar now has a CSV export for the active day, week, or month view.
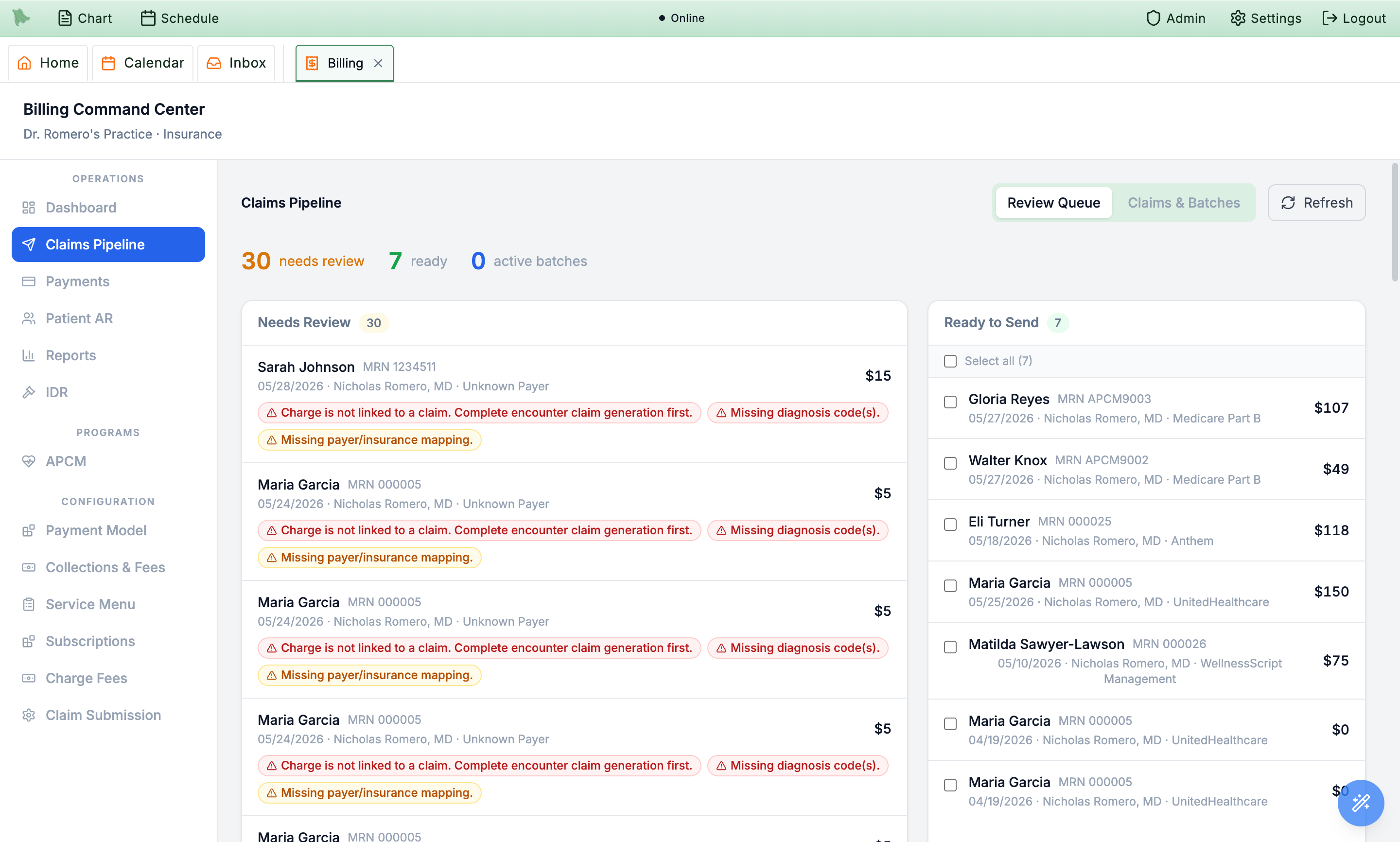
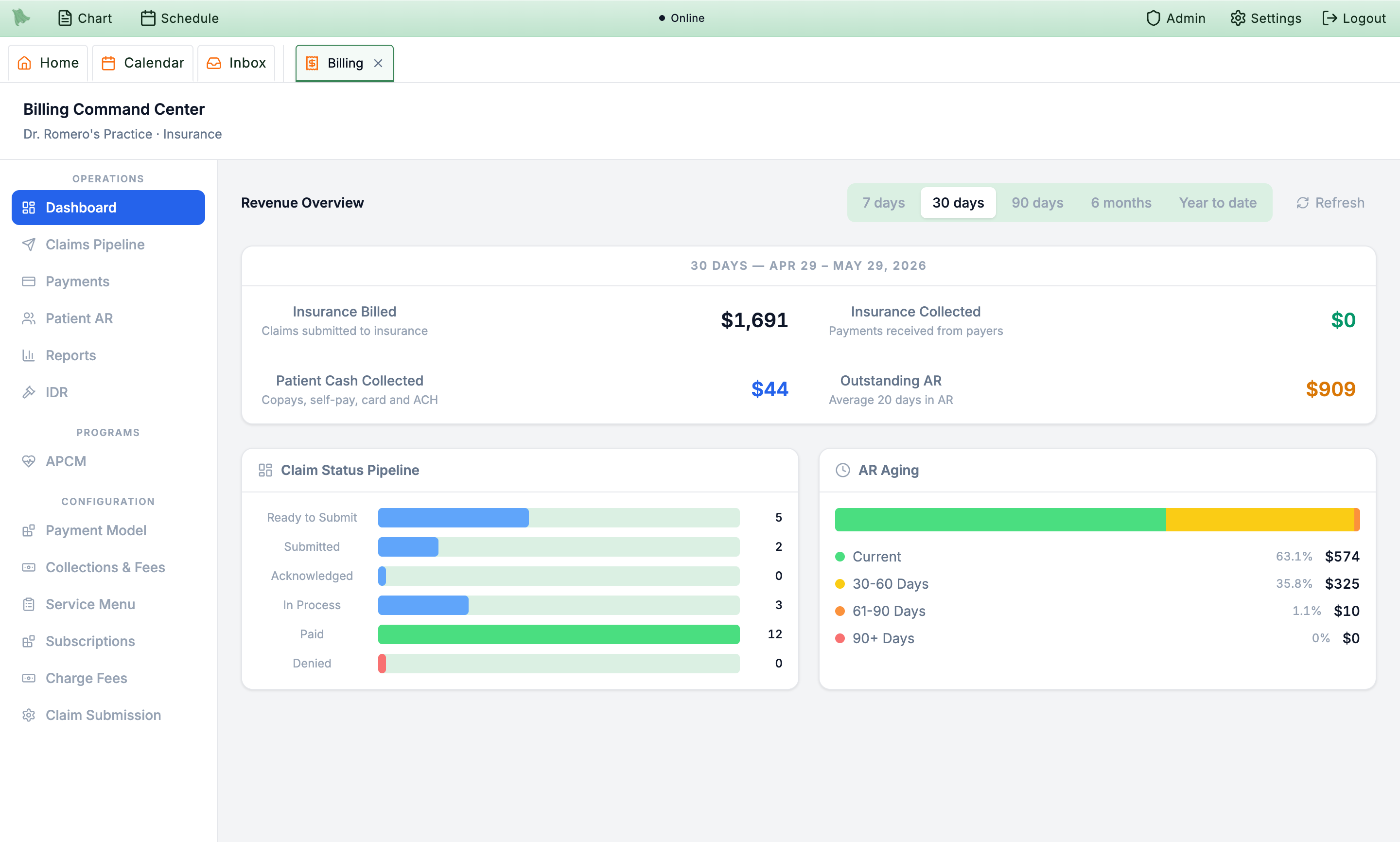
Stuck claims 30+ daysClaims pipeline now flags active claims with no recent claim activity.
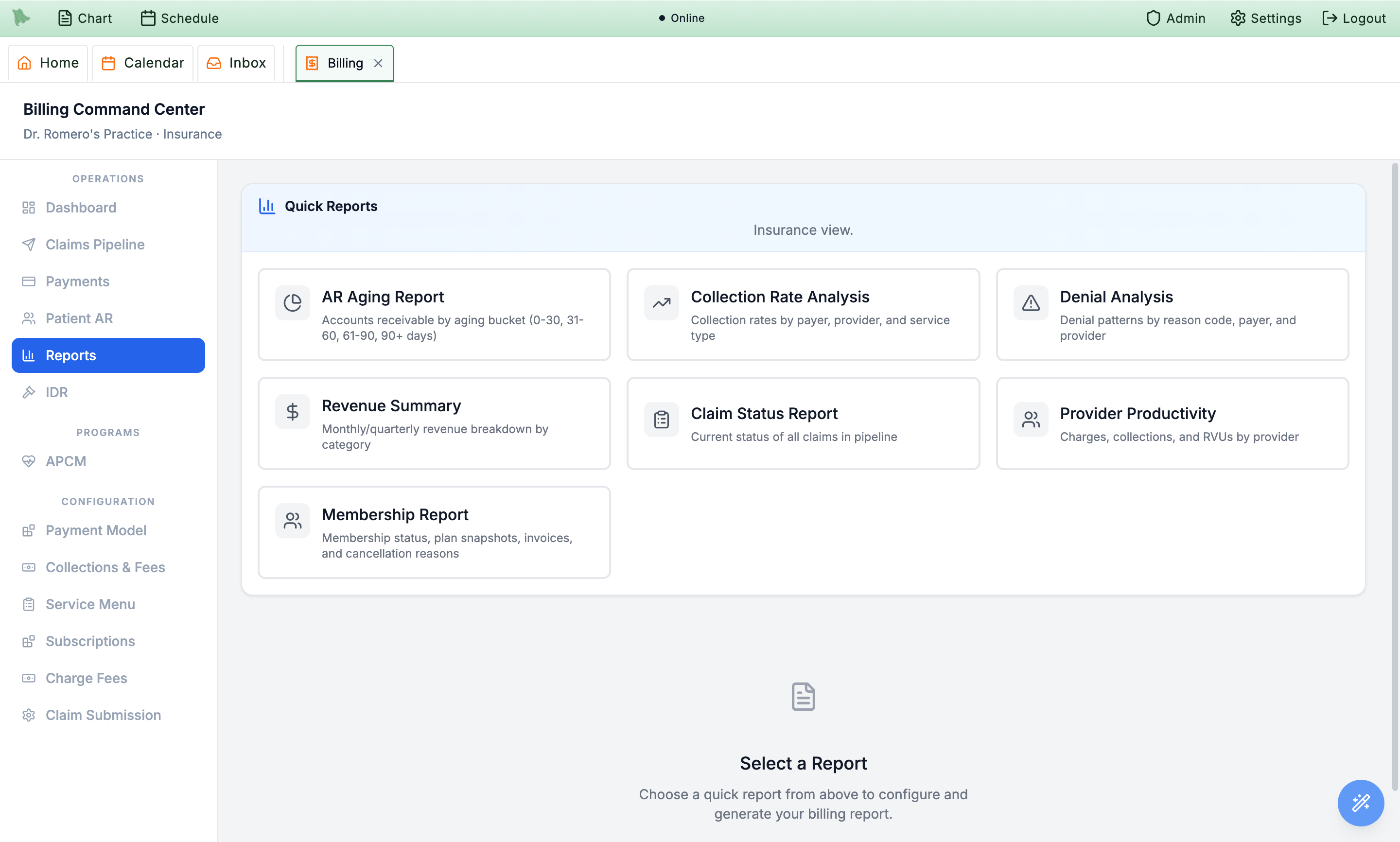
Denial rates by payerBilling reports now include payer-level denied ÷ total claim rates.
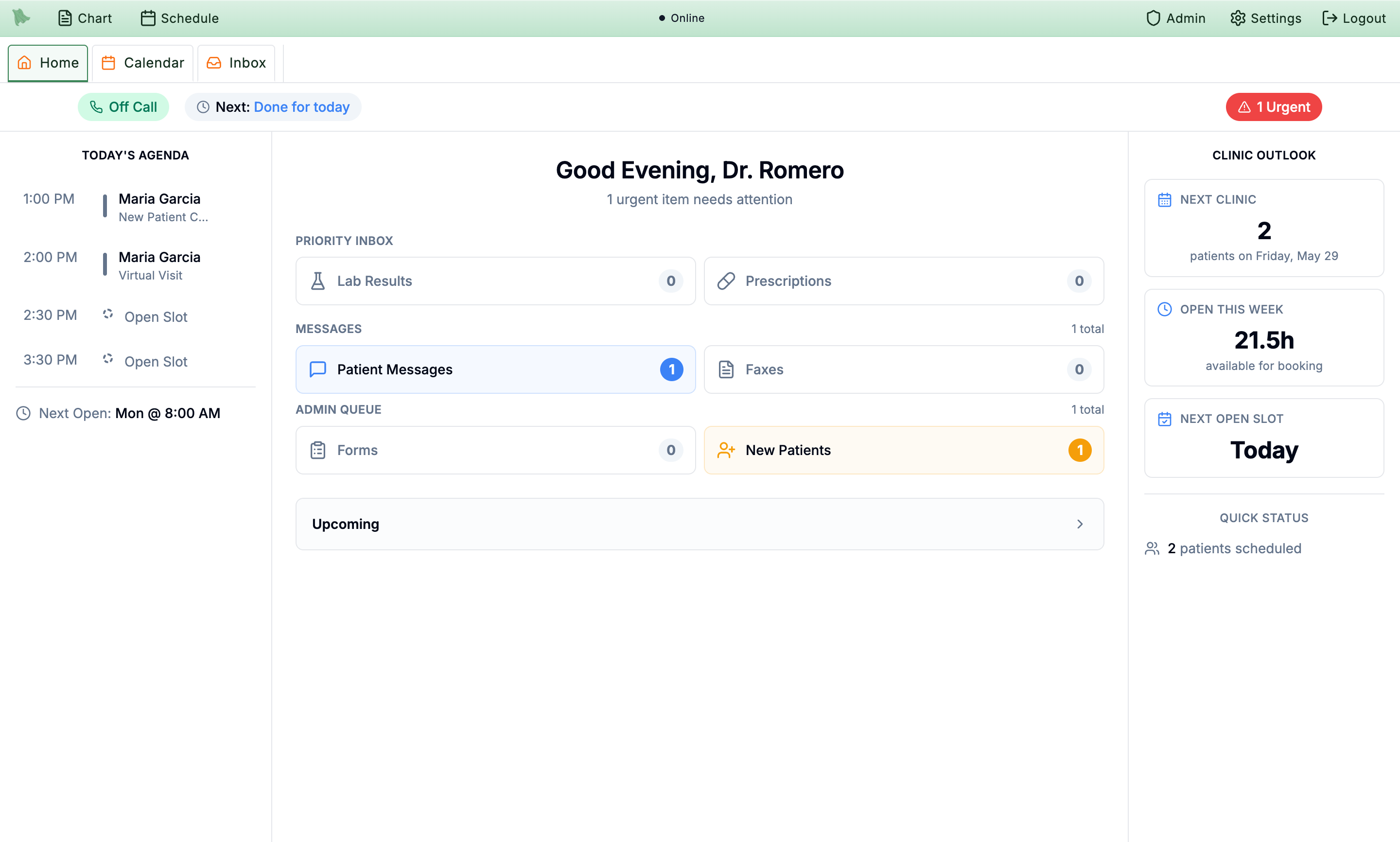
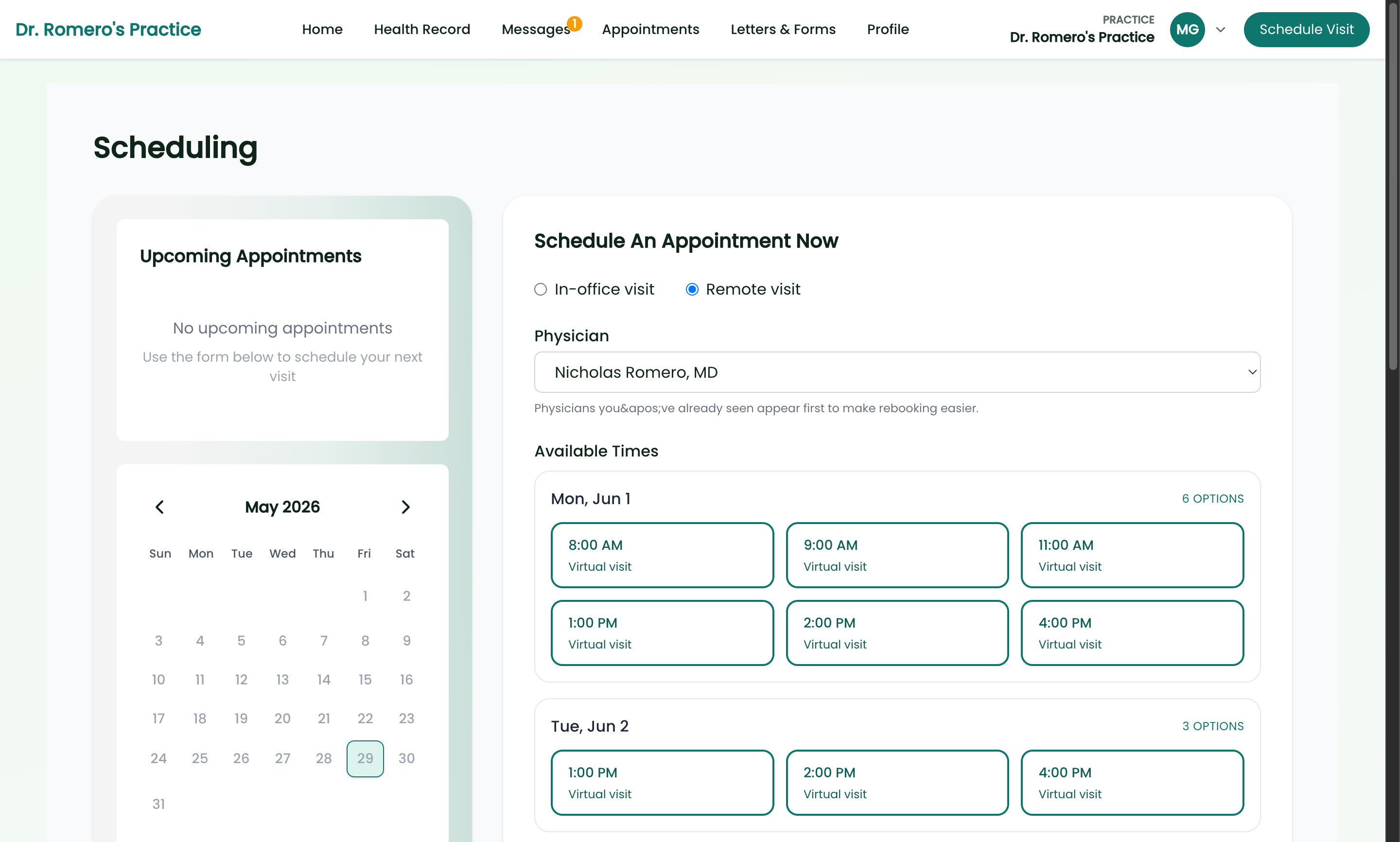
Scheduling gapsClinic Outlook now summarizes current and upcoming open-slot gaps.
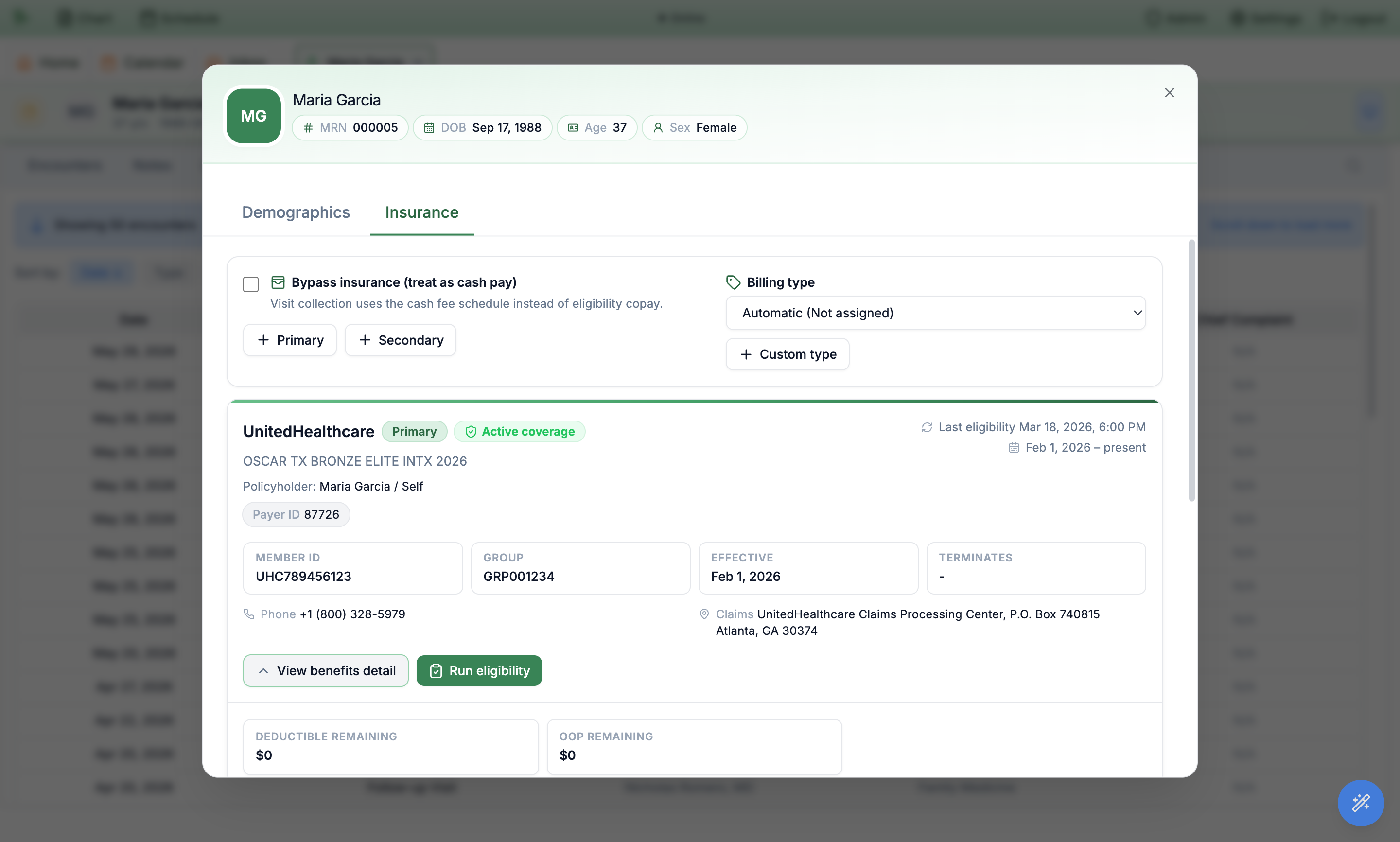
Inactive coverage warningsDay-view appointments now show non-blocking inactive coverage warnings.
Patient-responsibility estimateSaved eligibility benefits now auto-estimate the patient's portion per visit type.
Two-way textingReplies in an [SMS] thread now send a real text back to the patient.
Instant SMS answersCommon patient questions get an on-brand auto-answer before reaching your inbox.
Authorization trackingManage auths, track units used vs. remaining, and get alerts before they expire.
Appointment confirmationsPatients text CONFIRM and the calendar shows the visit as Confirmed.
Denial trends & spike alertsDenial data now trends over time with spike alerts and payer/provider patterns.